Detailed instructions are on the form. Signature of Member.
 Medical Claim Form Anthem Blue Cross Fill Out And Sign Printable Pdf Template Signnow
Medical Claim Form Anthem Blue Cross Fill Out And Sign Printable Pdf Template Signnow
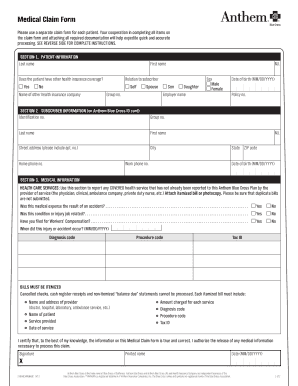
Last name First name MI.
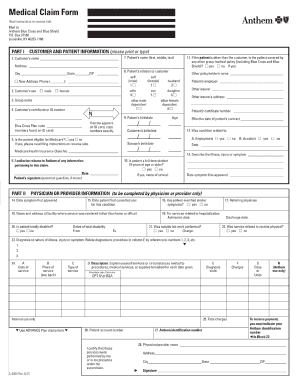
Anthem blue cross reimbursement form. On the Forms page scroll down to Request Reimbursement and click the blue Start a Claim button. Street address please include apt. Practice Profile Update Form.
Request For Reimbursement Anthem Blue Cross and Blue Shield Anthem Blue Cross and Blue Shield Supporting Documentation Employee Certification COVA Health FSA Reimbursement Form Created Date 7172017 32846 PM. SECTION 2UBSCRIBER INFORMATION S on Anthem Blue Cross and Blue Shield ID card Identification no. Medicaid only BCCHP and MMAI Medicaid Service Authorization Dispute Resolution Request Form.
Any missing or incomplete information may result in delay of payment or the form being returned. Medicaid Claims Inquiry or Dispute Request Form. Anthem Blue Cross and Blue Shield Healthcare Solutions is the trade name of Community Care Health Plan of Nevada Inc an independent licensee of the Blue Cross and Blue Shield Association.
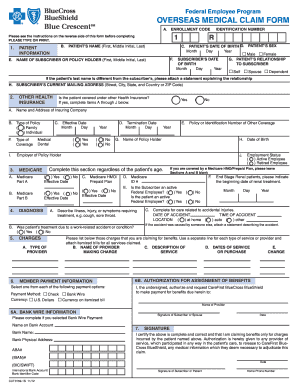
I am requesting reimbursement for Medicare Part B premium expenses I incurred while a member of the Blue Cross and Blue Shield Service Benefit Plan. Send the completed State of New Hampshire Home Exercise Equipment Reimbursement Form and photocopy of the original receipt to. If you take advantage of Service Benefit Plan dental benefits you will need to complete and file a claim form for reimbursement.
M edicare Reimbursement Account MRA Pay Me Back Claim Form. Independent licensee of the Blue Cross Association. I have notwill not seek reimbursement of this.
Form Title Networks Expedited Pre-service Clinical Appeal Form. In the event of an erroneous or excess reimbursement i understand i am required to reimburse the plan for the improperly paid amount. MCS Notification of Delivery Form.
Health Plan Name Member Name First Last Street Address City State ZIP Patient Information Patient Name First Last. Availity LLC is an independent company providing administrative support services on behalf of Anthem Blue Cross and Blue Shield. If your pharmacy is willing to accept assignment do not complete this form.
Send the completed Fitness Reimbursement Form and original receipt to. An incomplete form may delay your reimbursement. Sign and date the form when completed and keep a copy for your records form will not be returned.
17P Prior Authorization Form. Box 533 North Haven CT 06473-0533 Fitness Reimbursement Program 35648MUMENABS Rev. MemberSubscriber Information See your prescription drug ID card.
No City State ZIP code Home phone no. Anthem blue cross is the trade name of blue cross of california. Follow the instructions on the Get Reimbursed page and click the blue Get Started button when you are ready to begin your online claim.
Medical Injectables Prior Authorization. Claims Department Anthem Blue Cross and Blue Shield PO. Claims Department Anthem Blue Cross and Blue Shield PO.
If you have any questions call the number on the back of your Blue Cross ID card or contact us. Box 533 North Haven CT 06473-0533 4. HMO products underwritten by HMO Colorado Inc.
Keep a copy for your records. You have until December 31 of the following benefit year to submit your claim for reimbursement. AT7202 201201 Request for Reimbursement Dependent Care Flexible Spending Account Anthem Blue Cross and Blue Shield is the trade name of.
Also have a fitness center employee sign the bottom of the form. English Health Benefits Election Form SF 2809 Form. A new fcmv form will need to be completed each year or when you attend a new f tness center.
Blue View VisionSM Reimbursement Form Please complete the following steps prior to submitting the claim form to Blue View Vision. Date the form when completed. ANTHEM is a registered trademark of Anthem Insurance Companies Inc.
I authorize the release of any medical information necessary to process this claim. Claims Department Anthem Blue Cross and Blue Shield PO. PCP Change Request form Spanish.
Rocky Mountain Hospital and Medical Service Inc. Anthem Blue Cross is the trade name of Blue Cross of California. Instructions are on the back of the form.
I certify that to the best of my knowledge the information on this Member Claim Form is true and correct. By completing this form I recognize that reimbursement will be paid directly to me and that assignment of these benefits to a pharmacy or any other party is void. I certify that the information on this form is accurate and complete.
Prescription Drug Reimbursement Form See the back for instructions. Mail your completed Fitness Reimbursement Form Fitness Reimbursement Program Log Card and original receipts to. Box 533 North Haven CT 064730533 5.
Please complete and send this form to Blue View. PCP Change Request form English. The Blue Cross and Blue Shield names and symbols are registered marks of the Blue Cross and Blue Shield Association.
Browse commonly requested forms to find and download the one you need for various topics including pharmacy enrollment claims and more. To submit by mail or fax use the form below. Complete the Fitness Reimbursement Form.
Date If allowed by law you may assign the payment of this claim to your pharmacy. Medicaid only BCCHP and MMAI. We will not return the form 4.
Anthem Medical Claim Form Fill Online Printable Fillable Blank Pdffiller
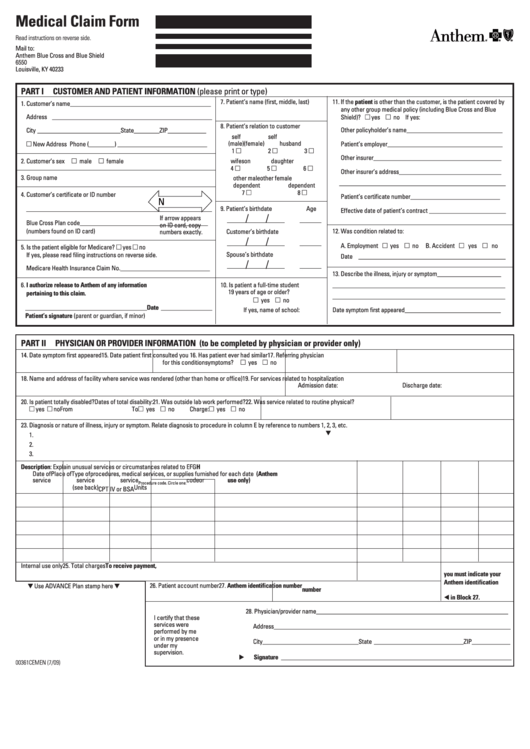 Form 00361 Medical Claim Form Anthem Blue Cross And Blue Shield 2009 Printable Pdf Download
Form 00361 Medical Claim Form Anthem Blue Cross And Blue Shield 2009 Printable Pdf Download
Https Www Anthem Com Ca Health Insurance Nsecurepdf English Ca Member Claim Form Pdf
Http Louisville Edu Hr Forms Anthem Major Medical Claim
Https Www Mpiphp Org Assets Files Forms Claims English Ca Member Claim Form Pdf
 19 Printable Medical Claim Form Blue Cross Blue Shield Templates Fillable Samples In Pdf Word To Download Pdffiller
19 Printable Medical Claim Form Blue Cross Blue Shield Templates Fillable Samples In Pdf Word To Download Pdffiller
 Get 10 How To File A Claim With Anthem Blue Cross California Images Penny Matrix
Get 10 How To File A Claim With Anthem Blue Cross California Images Penny Matrix
 Fillable Online Sjeccd Supporting Documents Uci Accounting And Fiscal Services Fax Email Print Pdffiller
Fillable Online Sjeccd Supporting Documents Uci Accounting And Fiscal Services Fax Email Print Pdffiller
 24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
Https Www Frederick K12 Va Us Userfiles Servers Server 135851 File Staff Forms Hr Forms Anthem Reimbursement Claim 061016 Pdf
Https Www Anthem Com Provider Noapplication F5 S2 T0 Pw E234048 Pdf Refer Ahpprovider State Ct
 21 Printable Blue Cross Blue Shield Health Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
21 Printable Blue Cross Blue Shield Health Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
 Anthem Blue Cross Claims Fill Online Printable Fillable Blank Pdffiller
Anthem Blue Cross Claims Fill Online Printable Fillable Blank Pdffiller
Https Www Anthem Com Provider Noapplication F0 S0 T0 Pw E195001 Pdf Refer Ahpfooter Na Cova




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.